
Rh Immune Globulin helps prevent Hemolytic Disease of the Fetus/Newborn, but why is it so hard to decide how much to give?

Dr. Jessica Hudson
RhIG to the Rescue!
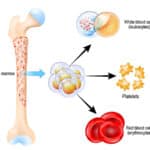
The good news: RhIG, when given at the right time and in the right dose, does a wonderful job at preventing formation of anti-D in at-risk moms. In fact, in 99% of RhD-negative moms, the process is really, really simple. That mom gets RhIG at two times: First, at her 28 week OB visit, when we give her the contents of one prefilled syringe (or “vial”) of RhIG, and second, when we give her a second vial after she delivers an RhD-positive baby. Easy, right?
The BAD News
The bad news is what happens in the 1% of moms when things are not so simple. These are the RhD-negative moms who have a larger-than-normal exposure to their baby’s blood, and as a result, might need more than one vial of RhIG. Numerous studies have shown that those calculations (yes, there will be math in this situation!) are not always done accurately. This podcast is an attempt to simplify the calculations and make them memorable for learners.
This Episode is a New Start
Two things are unique about this episode. First, you are going to get to hear me in a live teaching session with one of my residents, Dr. Jessica Hudson, a third-year pathology resident at Loma Linda University. Second, this is the first episode where I am using a previous “Transfusion Medicine Question of the Day” from TransfusionNews.com as a starting point. If you aren’t signed up for the thrice-weekly, totally FREE Question of the Day series, you really should be! In fact, go there now and sign up!
The question you see below was written by Lorraine Blagg, MA, MLS(ASCP), SBB from Johns Hopkins, and is displayed here courtesy of TransfusionNews.com.
Dr. Jessica Hudson
RhIG to the Rescue!
The good news: RhIG, when given at the right time and in the right dose, does a wonderful job at preventing formation of anti-D in at-risk moms. In fact, in 99% of RhD-negative moms, the process is really, really simple. That mom gets RhIG at two times: First, at her 28 week OB visit, when we give her the contents of one prefilled syringe (or “vial”) of RhIG, and second, when we give her a second vial after she delivers an RhD-positive baby. Easy, right?
The BAD News
The bad news is what happens in the 1% of moms when things are not so simple. These are the RhD-negative moms who have a larger-than-normal exposure to their baby’s blood, and as a result, might need more than one vial of RhIG. Numerous studies have shown that those calculations (yes, there will be math in this situation!) are not always done accurately. This podcast is an attempt to simplify the calculations and make them memorable for learners.
This Episode is a New Start
Two things are unique about this episode. First, you are going to get to hear me in a live teaching session with one of my residents, Dr. Jessica Hudson, a third-year pathology resident at Loma Linda University. Second, this is the first episode where I am using a previous “Transfusion Medicine Question of the Day” from TransfusionNews.com as a starting point. If you aren’t signed up for the thrice-weekly, totally FREE Question of the Day series, you really should be!
About My Guest:
Jessica Hudson MD is, as of this recording, a third-year pathology resident at Loma Linda University in Loma Linda, CA. She is a Southern California native who loves all things adventure and Transfusion Medicine. She and her husband enjoy snowboarding, line dancing, singing in the car, as well as everything related to “the classics” (Star Wars, Lord of the Rings, and Harry Potter).
DISCLAIMER: The opinions expressed on this episode are those of my guest and I alone, and do not reflect those of the organizations with which either of us is affiliated. Neither Dr. Hudson nor I have any relevant financial disclosures.
Further Reading:
- A Brief History of the Use of RhIG, by Lynsi Rahorst from the New York Blood Center (Lynsi is also a BBGuy Associate Editor).
Thanks to:
- Dr. Jessica Hudson: For being the first resident to be a part of this podcast, and for trusting me not to embarrass her (not sure I succeeded, but I tried!).
Music Credit
Music for this episode includes “Cuando te invade el temor” and “Reflejo,” both by Mar Virtual via the Free Music Archive. Click the image below for permissions and license details.![]()











I was wondering if the blood volume of some Moms , and of other patients in general, Is underestimated because of blood vessel characteristics other than height and weight. I cashiered for a long time and I think the veins in my legs are wider than they need to be, and maybe they have multiple curves in them to increase the length, in effect. I wonder if enlarged veins can mimic 20 pounds of additional weight as far as blood volume. Does that make sense?
Good to hear the new upload today!
Estimates of blood volume are just that, Gina. They are best guesses, and certainly individual variation makes things less than perfect. I talked about how we always “add 1 vial” at the end of the calculation. That’s in part because the K-B test is not a wonderful test, but also because we are estimating to an extent on mom’s blood volume. The extra dose is to try to add a cushion of safety.
-Joe
Sounds good to me. 🙂 Thank you for all your work and time.
Hi Dr. Chaffin,
So glad to get a new episode! I’m a pathology resident from Canada and I wanted to say I really appreciate all the education you provide!
I’ve subscribed and rated on spotify – hopefully more learners can find your podcast!
Calvin
Hi Calvin! Thanks so much for taking the time to write (and for the rating and review on Spotify). I’m very glad you enjoy the podcast.
-Joe
Thanks for the great review while studying for the SBB. Listening to your podcast is so much more engaging that reading the Tech Manual!
Hey now, Allison, we can’t be bashing on the Tech Manual! :^] I’m glad the episode was helpful to you in your review. Best of luck on the SBB!
-Joe
I thought you might find this veterinary transfusion interview interesting. I hope it gives you a surprise or a chuckle. It’s brief. 🦅🦅
https://open.spotify.com/episode/2OTtwz1ShM0ZhIxwFD0FKT?si=HeGNg4W_S3W69ZDXcQtamw
Thank you.
When they said chickens have 20 ? blood types I laughed pretty hard.
Enjoy your podcasts.
42 years in transfusion medicine/donor center MD this case is unique.
A recent event.
Massive FMH or not.
35 yr old G1P0, 63 kg, prenatal Hct 35%, blood type O, D negative, antibody screen (AbS) negative, delivered 3.1 kg male infant , blood type O pos, DAT neg, AbS negative. FMH screen.
KB 5.9 %, Reviewed KB slide for fetal cells, typical fetal cell pattern.
So we investigated further.
Healthy male infant
No obstetrical complications.
Repeat KB 5% fetal cells
neonate. Hgb 16 gm/dl
Referred for flow cytometry 5% fetal cell.
Patient received 10 300ug doses IM.
Then I saw your new podcast!
Oops patient receive antenatal RHIg 300 ug.
I can’t give medical advice on specific cases on the website, for obvious reasons, but as I mentioned in the podcast, when you find yourself saying something like, “That’s a LOT of RhIG. Like, a LOT!”, and the amount would suggest a fetomaternal hemorrhage (FMH) roughly equal to the baby’s total blood volume, further investigation might be warranted. Such a huge FMH is not impossible, I guess, if the hemorrhage was chronic, but if the baby’s hemoglobin was near normal, it would really make me wonder. The further investigation and management would of course be at the discretion and direction of your local medical director.
-Joe
Love your Podcast (german Anesthesiologist)! Learn a lot and am very glad to have your voice coming out of my car speakers again: welcome back 🙂
The current episode is fantastic. Great format! Interviews are good, teaching is as well 🙂 Great listen! Keep up the great work!
Hi Simon! I’m so honored that you would take the time to listen! Thanks for the kind words.
-Joe
What about moms who are Du positive, they would have a false positive rosette test. Would a KB stain still be performed since there are some Du positive people who can be sensitized to anti-D?
By the way I absolutely love your podcasts! Thank you!
Mirella, moms with weak D (the term “Du” is no longer used) would indeed have a positive rosette test, since the test couldn’t discriminate between mom’s and baby’s D+ RBCs. Whether or not you do a quantitative test like a Kleihauer-Betke would ideally be determined by the results of mom’s RHD genotype test (for more on this recommended test in weak D moms, see 090CE: RHD Genotyping; We Can Do Better! with Sue Johnson or 005: Rh Genotyping with Connie Westhoff). In general, if mom has one of the common forms of weak D (e.g., types 1, 2, 3, and probably 4.0 and 4.1), then she is treated as if she were RhD+, and no KB or other quantitative test is necessary. If her RHD genotype, however, was NOT one of those listed above, most would manage her just like an RhD-negative mom, and she would need a quantitative test if her baby were RhD-positive. I hope that helps.
-Joe
Great episode! I’ll probly listen to it several times.I have a question about irradiation: Should patient’s who have had Hodgkin lymphoma have irradiated blood products? They weren’t mentioned in the “radioactive” section, but it is mentioned in the Canadian and British guidelines
https://nacblood.ca/en/resource/recommendations-use-irradiated-blood-components-canada
Thanks
Subject: Fetomaternal hemorrhage
Message: Dear Joe,
Chris González texting. Love you man! Love your podcasts as do all my residents. Re: fetomaternal hemorrhage… I have had several cases of very high fmh volumes nearly as large as the baby’s predicted blood volume… probably due to a chronic fmh. The baby was profoundly anemic. Below is a link to a similar published case report. For my patient I gave a large volume of RhIG but wondered if the antecedent chronic bleed would have already alloimmunized Mom in spite of a 28 week RhIG prophylaxis. Unfortunately I don’t have follow up. Call me if you need or want more details. Keep up your awesome work! You are my hero!!
With highest and fondest regards,
Chris
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3653511/
Hi Chris! You are too kind. Thank you for the feedback and the example of a person with a real higher KB result that required lots of RhIG. I understand, and I’ve had a couple of others say similar things (in fact, an April 2023 article in AJCP from the brilliant folks at UCLA described something similar; see https://doi.org/10.1093/ajcp/aqad011). Obviously it CAN happen that a sky-high KB result is real; my personal experience is that more of them are false-positives. Thanks for writing.
-Joe
For those struggling with the citric acid kleihauer, we have automated it on the Leica ST4020 linear stainer using the Merk kit at room temperature, correlated with flow cytometry. Melbourne Australia.