
“Anti-CD47 is here, and it’s really going to mess up our testing!” Connie Westhoff explains how we can accurately test our patients’ blood.
NOTE: Continuing Education credit for this episode has expired. See below for details.

Dr. Connie Westhoff
You Think DARA was Bad?
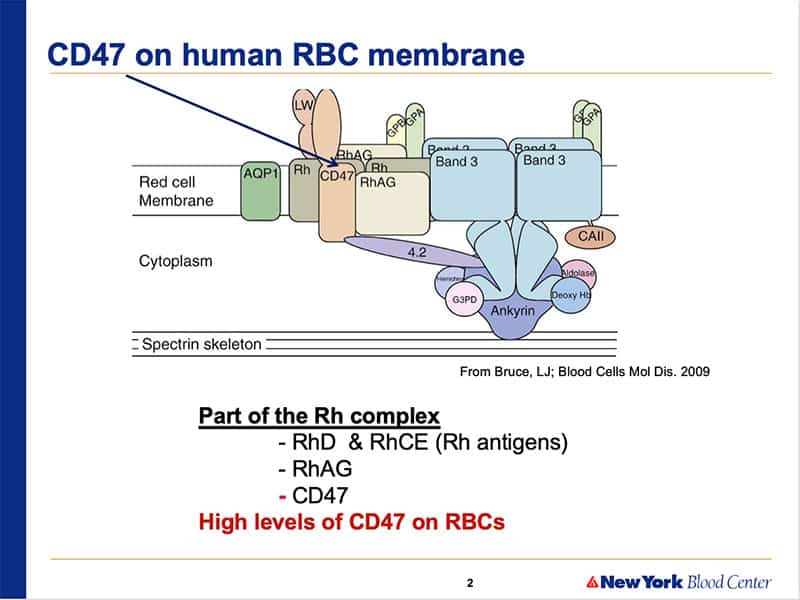
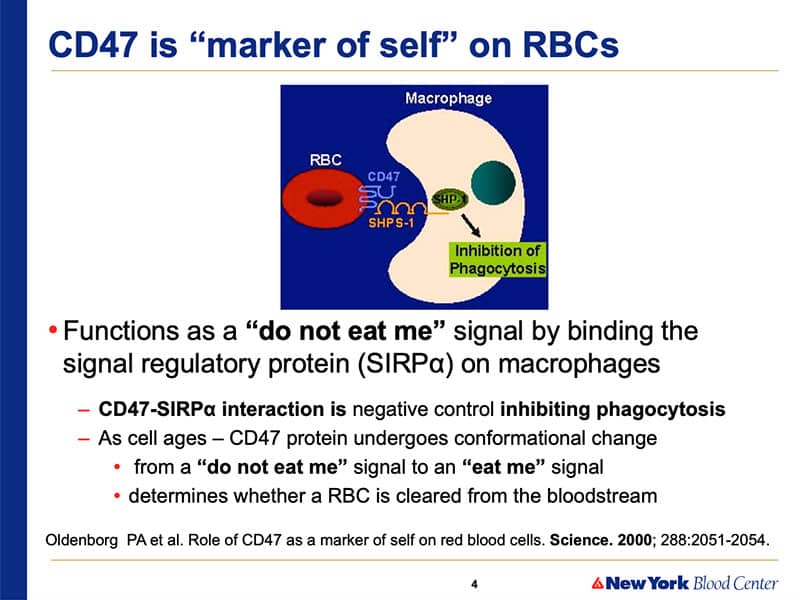
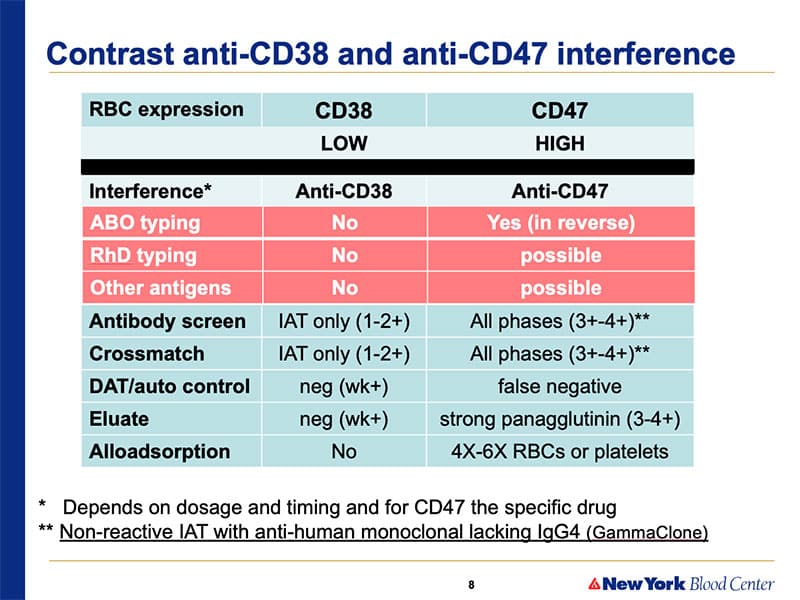
Almost since DARA was introduced, there have been rumblings and rumors about a new chemotherapeutic agent, anti-CD47, that would have FAR greater impact on the routine tests performed in blood banks everywhere. Well, anti-CD47 is now in active trials in several places in the U.S., and it looks like our fears have been realized: This drug heavily coats red blood cells, and causes major problems with ABO testing, antibody detection tests, and platelet compatibility tests.
Connie to the Rescue!
Dr. Connie Westhoff and her group from the New York Blood Center report on their experience with a series of four patients on anti-CD47 in the February 2019 journal, “Transfusion” (see link below). Connie is here to share with us what works, what clearly does NOT work (Hello, DTT!), and proactive steps clinicians and blood bankers can take to make things much easier for us and the patients on this medication (Hello, pre-treatment genotyping!).
Dr. Connie Westhoff
You Think DARA was Bad?
Almost since DARA was introduced, there have been rumblings and rumors about a new chemotherapeutic agent, anti-CD47, that would have FAR greater impact on the routine tests performed in blood banks everywhere. Well, anti-CD47 is now in active trials in several places in the U.S., and it looks like our fears have been realized: This drug heavily coats red blood cells, and causes major problems with ABO testing, antibody detection tests, and platelet compatibility tests.
Connie to the Rescue!
Dr. Connie Westhoff and her group from the New York Blood Center report on their experience with a series of four patients on anti-CD47 in the February 2019 journal, “Transfusion” (see link below). Connie is here to share with us what works, what clearly does NOT work (Hello, DTT!), and proactive steps clinicians and blood bankers can take to make things much easier for us and the patients on this medication (Hello, pre-treatment genotyping!).
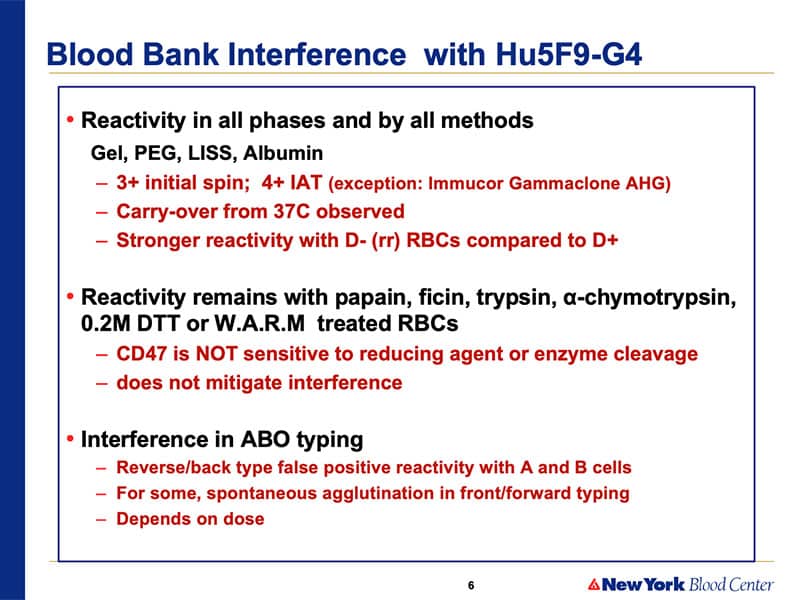
Our first thing was to try and remove it from the red cells like it works so well for DARA! DTT, enzymes… So we threw the kitchen sink at CD47 and nothing “stuck,” so to speak. DTT doesn’t destroy the epitope, enzymes don’t destroy the epitope, papain, chymotrypsin, ficin; none of those things. W.A.R.M. reagent; nothing will denature the CD47 on the test red cells.
About My Guest:
Connie Westhoff, SBB, PhD is the Executive Scientific Director of the Laboratory for Immunohematology and Genomics at the New York Blood Center and the National Center of Blood Group Genomics in Kansas City. Dr. Westhoff lectures nationally and internationally, and has published more than 100 scientific papers and numerous book chapters. She is an Associate Editor for the Immunohematology and Genomics Section of the AABB journal “Transfusion,” and is also an editor of several editions of the AABB “Technical Manual” (my recommended textbook for those learning Transfusion Medicine). Connie is also an avid supporter of the National Blood Foundation and one of the original inductees to the National Blood Foundation Hall of Fame.
Check out Connie’s previous appearance on the podcast, where she describes how to deal with serologic Weak D with molecular testing.
Continuing Education Expired
This podcast episode offered continuing education credit for two years from its release date, but is no longer eligible for such credit.
To find Blood Bank Guy Essentials Podcast episodes with active continuing education opportunities, Click here or visit Transfusion News Continuing Education on Wiley Health Learning.
DISCLAIMER: The opinions expressed in this episode are those of my guest and I alone. Those opinions do not necessarily reflect those of the organizations with which either of us is affiliated. This podcast does not constitute formal medical advice. Please discuss all medical issues and decisions with your local health care providers. Neither Dr. Westhoff nor I have any relevant financial disclosures.
The images below are generously provided by Dr. Connie Westhoff.
Further Reading:
- Article discussed extensively in this interview: Velliquette RW et al. Monoclonal anti‐CD47 interference in red cell and platelet testing. Transfusion 2019
Music Credit
Music for this episode includes “Cuando te invade el temor” and “Reflejo,” both by Mar Virtual via the Free Music Archive. Click the image below for permissions and license details.![]()











I am a bit lost with the historically labeled units. If we have previous RBC antigen profile (RHs,Kk,Lea,b,fya,b,jka,b,MNSs)of a patient and request historically labeled units from blood center, the cost will the less? Can we do this every time that patient requires transfusion without sending specimens to reference lab for work up if the patient is on anti CD47 or has warm auto? The historic labeled is for blood center, not for hospitals? Or it works both ways?
This is a VERY big topic, and the answers are going to be very individualized, both for blood suppliers and for transfusion services. For cost, every blood supplier (blood center) will have to determine the cost for this service. I can’t tell you what each center will decide, unfortunately, but it’s hard to imagine a cost for units negative by historical testing being MORE than the cost for units that are currently tested by various mechanisms. Whether it will be substantially less, however, is something I can’t say. As far as the clinical USE of historically tested units, that decision will be up to the transfusion service medical director in terms of how often a new workup needs to be done if the patient is being genotypically matched for antigen types, for example. It could potentially save some workups, of course, but the facility medical director has final say in that discussion. Sorry I can’t be more specific, but there’s no universal answer.
-Joe
Have there been any additional research studies that explore Anti-CD47 interference? Or is the information and results for the 4 patients Dr. Westhoff the only published studies available on this topic?
I was wondering…If a patient was taking this medication and transfused incompatible RBCS, could the anti-CD-47 cover the RBCs so well the RBC antigen sites would be inaccessible to the immune system preventing a hemolytic transfusion reaction….
And by the way, why aren’t RBCs coated with antibody removed by the spleen and Kupfer cells in the liver. ??
By the way… thank you very much for doing this… I have yet to hear a bad interview and the informal presentation gives me time to think…… perhaps not a good thing ;o)
Both are great questions, Kip, and I don’t have the answers. I’ll see if Dr. Westhoff has any further insight. Meanwhile, thanks for the kind words.
-Joe
Perhaps the anti-CD47 is an IgG4 and escapes detection by the reticuloendothelial system?
I’m a bit confused about the use of PEG. Was it just referring to PEG Adsorptions, or should we also stay away from using PEG in the neat serum? Also, what is meant by “proper controls” and why were they invalid? We’ve had 2 anti-CD47 cases recently that were completely negative in PEG with neat serum, but positive at 37 degrees using LISS with neat serum. Are the PEG results valid?
I’m disappointed to see this episode is no longer available as a link on your website. We are soon to be receiving samples for pre-transfusion testing from a hospital where they are in a trial using CD47. We wanted to use this podcast to help educate our staff. Other than directing everyone to Apple podcast or Spotify, would it be possible to repost this episode?
I listened to this when it first came out and it was very helpful.
Thank you.
Renee, the episode is still available, and anyone can listen to it using the player right here on the page! It’s just that the continuing education credit has expired (Wiley Health Learning puts a two-year limit on when the CE expires, and I don’t control that). The audio, transcript, slides, etc, are still present and your staff can absolutely still use them. I hope that helps.
-Joe
Thank you for the quick response. The problem was on our end. One of our PCs did not display the player. It only said the program was not available.
I’m so glad it’s still here. Thanks again Joe. Renee
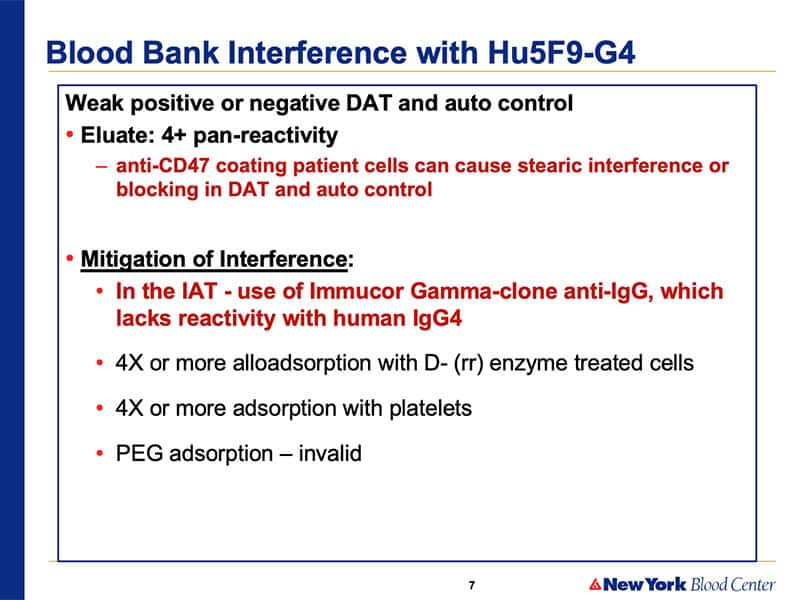
What AHG are they using for IAT phase? I am a student researching anti-CD47 and i’m a bit confused since our lab uses Immucor gamma-clone anti-IgG, I thought it was a standard. Do most anti-IgG on the market detect IgG4? Great talk!